
Ask anyone who has had a kidney stone and they will tell you it is the worst pain of their life. If you are reading this with a sharp pain gripping one side of your back, you want three answers fast: how do I make it stop, will I need surgery, and will it happen again? After 30 years of treating stones across Delhi and Gurgaon, here is the honest version. Most stones can be handled without surgery, the pain can be controlled quickly, and most of the next ones can be prevented.
The pain that drops you to your knees
A kidney stone usually starts as sharp, cramping pain on one side of your back or stomach. It comes in waves: builds to a peak, eases, then builds again. No position helps, and many people feel sick or throw up. This happens when a stone slips into the urine tube and the kidney cramps hard against the blockage, the way any muscle cramps when it pushes against something stuck. Doctors call it renal colic, a useful word to know, because saying it tells a doctor exactly what you are feeling.

Stone pain is one-sided: it runs from the side of the lower back around toward the front.
The vomiting is what confuses people. Because the stomach feels involved, many assume it is indigestion, gas or food poisoning, reach for stomach medicine, and wait. That delay is the real danger. Two clues tell you this is not your stomach. First, the side: a stone almost always hurts on one side only, left or right, while a stomach problem sits across the middle or the whole belly. Second, nothing helps: the pain does not ease however you lie down, sit up, or turn, it just keeps coming in waves. If both are true, treat it as a stone until a doctor proves otherwise.
For the pain, a doctor can give you the right painkiller. But a painkiller only quiets the pain. It does nothing to the stone. The stone still has to pass or be treated.
Go straight to a hospital, do not wait for an appointment if the pain comes with fever or chills, you are passing little or no urine, or you cannot stop vomiting. A stone on its own is rarely dangerous. But a blocked, infected kidney is serious: the infection can spread from the trapped urine into your blood and make you very ill fast. The medical name for that is sepsis.
"Do I need surgery?" The first thing everyone asks
Almost every patient asks me this in the first minute, so let me answer it plainly.
A small stone, the size of a grain of rice or smaller (under about half a centimetre), has a good chance of passing on its own in urine within six weeks, around 9 in 10. It has to travel down the ureter, the narrow tube, about the width of a straw, that carries urine from the kidney to the bladder. That tube is where a stone gets stuck and causes the worst pain. It can stretch a little for a small stone, but once a stone is bigger, the chance of passing on its own drops fast.
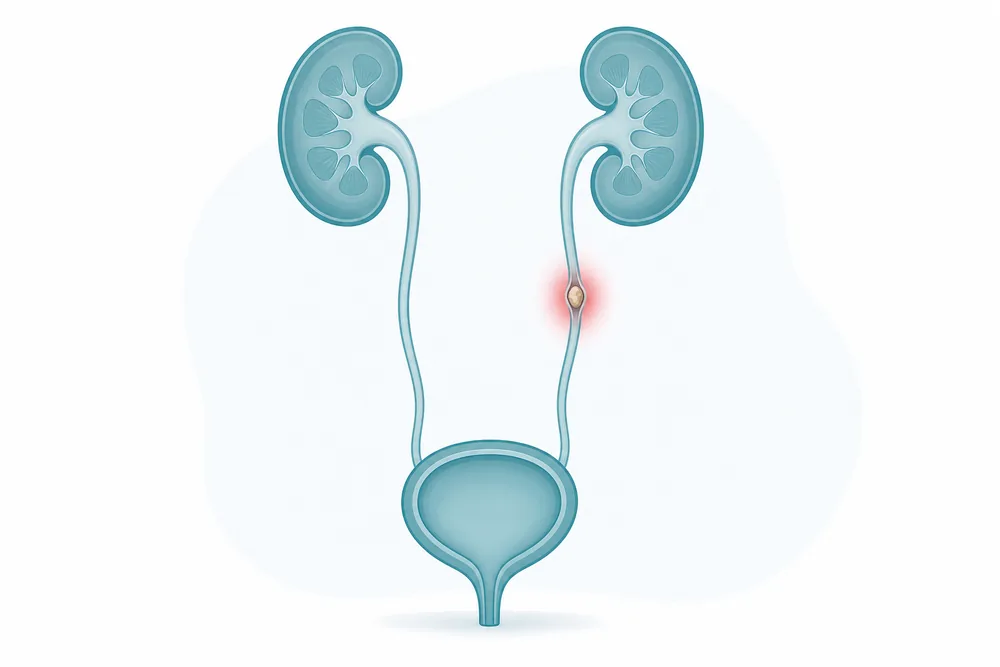
Urine travels kidney to bladder through the ureter, a tube about as wide as a straw. A stone gets stuck there.
To help a small stone on its way, you may be offered a "stone-passing medicine." It works by relaxing the ureter so the stone can slide down more easily. The medicine is called tamsulosin. To be straight about it: for most stones it makes little difference, though it can help a larger stone that is sitting low down near the bladder. It is not a magic cure, and it is no replacement for getting properly checked. Whether it is worth trying for you is something your doctor decides with you.
Even while we wait, I do not gamble with your kidney. If we are giving a stone time to come out, you have to be checked every five to seven days to make sure it is moving down and not quietly backing up urine behind it. If it is not moving after a week or ten days, or the kidney is swelling, it is safer to remove it surgically than to keep waiting.
"Honestly, everyone is scared of surgery. I do these procedures every day, and even I would be scared if it were me. So I understand the fear completely."
What reassures most people is this. Removing a stone today is usually not the big open operation people picture. In most cases we pass a very thin tube up the same passage urine comes out of, reach the stone, and break it with a laser, a focused beam of light that crumbles the stone into tiny pieces you then pass out in urine. There is no cut at all. This keyhole approach through the urine passage is called ureteroscopy. There is very little discomfort afterwards. Most patients go home the next day and are back at work within a day or two. A large stone is sometimes taken out instead through a small cut in the back, an operation doctors call PCNL. Even then it is just one extra day in hospital and a small wound that heals in about a week.
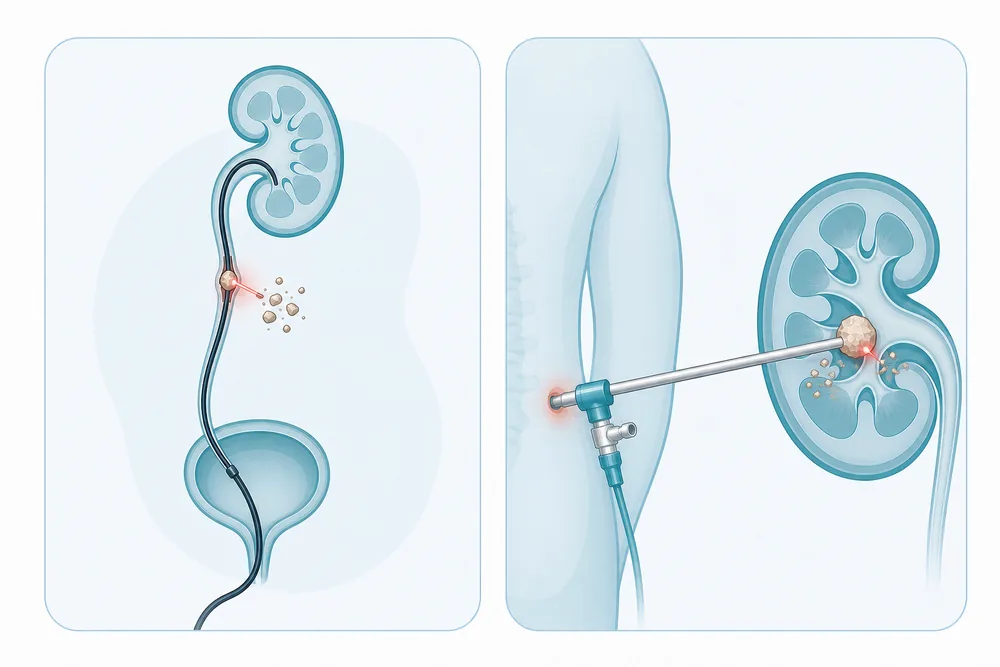
Two common treatments: a thin scope with a laser (no cut), or a small keyhole in the back for larger stones.
So with a small stone you often have a choice: wait it out, with up to six weeks of "let us see" and pain that can flare any time the stone moves, or have it removed now for quick relief. More and more people pick quick relief, because modern life does not allow weeks of uncertainty. I recently treated an airline pilot who was grounded the day a stone was found, because no airline wants a pilot in sudden pain mid-flight. He just said, "Now that I know it is there, take it out." I see the same with people in demanding jobs who cannot risk an attack at the wrong moment. For them, a quick procedure and a fast recovery are the sensible choice.
What does the surgery cost?
"And what does it cost?" is usually the next question, so let me be just as open about that. The price depends on which procedure you need. Ureteroscopy, the keyhole approach through the urine passage with no cut, costs less than PCNL, the one done through a small cut in the back. Which one is right for you comes down to the size of the stone and where it is sitting, so the number is not the same for everyone. At Holy Family Hospital, where I practise, stone-removal surgery comes to about ₹85,000 to ₹1.5 lakh, and that figure includes all the tests and scans, not only the procedure itself. One more thing that puts people at ease: because this is proper surgery with a hospital stay, most health insurance plans cover it.
What tests you actually need, and the mistake to avoid
The first test is an ultrasound, the same kind of scan used in pregnancy. It is quick, painless, and has no radiation, so it is the right place to start. But an ultrasound is only a first look. Spotting a stone is the beginning, not the end. We still need to check that there is no infection in the urine, see how the kidney is working, and usually do a CT scan (a detailed X-ray that shows the exact size and position of the stone) to plan properly. So the order is simple: ultrasound first, then a CT scan if a stone is found.
The common mistake I see is this: an ultrasound finds a stone, and then nobody follows it up properly. The patient is handed some medicine and sent home, with no one checking the size, the position, or whether the kidney is being harmed. That is how people get into trouble. If you are told you have a stone, get the full picture. Do not stop at the first scan.
One thing I do every single time I remove a stone: I send it to a testing lab to find out what it is made of. Your lab report will name the type, so it helps to know what those names mean. You might be surprised what we find:

The three kinds of stone. Calcium oxalate is by far the most common, about 9 in 10.
Knowing the type matters. If your stones keep coming back, it tells us exactly where to look and which medicine may help prevent the next one.
One practical tip: get your ultrasound done at a reliable centre. A clear, detailed report is the map your urologist uses to help you. A vague report sends everyone back to square one.
What is really causing your stones (it is simpler than you think)
People expect a complicated answer. Almost always, it is just this: not enough water.
Think of it like a glass of nimbu paani. Your body puts out a certain amount of salts in your urine every day, no matter what. If those salts are dissolved in only a little water, the urine is like over-concentrated nimbu paani, where the extra sugar will not dissolve and settles at the bottom as grit. That grit is how a stone begins. Now dissolve the same salts in a big jug of water. There is no grit at all, it all stays dissolved. Doctors call the watery, well-diluted urine you want dilute urine, and the dangerous over-strong kind concentrated urine. So the aim is simple: keep your urine dilute, watered down and pale.

Too little water leaves grit at the bottom, the start of a stone. Plenty of water keeps it all dissolved.
And it has to be every day, not just on the days you remember. I have seen very careful patients get a stone from a single bad afternoon.
"One man carried a water bottle everywhere and drank well all year. Then one afternoon he spent four hours shopping in Lajpat Nagar in the sun, sweating, drinking nothing. Those few hours of concentrated urine were enough to form the one tiny crystal that later caused all his trouble. It only takes one gap."
This is exactly why Delhi and Gurgaon see so many stones. They turn up far more in summer and the dry months, and they shoot up during fasting, for example through the Ramzan fasts in March and April, when people go all day without water. They are much less common in winter. The pattern is the same across Delhi and Gurgaon, and it climbs even higher in the hotter, drier parts of Rajasthan around Jodhpur and Bikaner, and in Gujarat. Hot weather plus too little water is the whole recipe.
The myths I correct every single week
Myth: "Stop all milk, paneer and calcium." This is the most harmful myth of all, so please do not do it. Cutting out calcium does not protect you. It backfires. When your body does not get enough calcium from food, it starts pulling calcium out of your bones instead, and that does double damage: it can still feed the stone, and it quietly weakens your bones. I often have to stop families from telling a patient to give up milk, and stop older women from throwing away their calcium tablets after a stone. Keep your normal calcium and dairy.
Myth: "Never eat tomato or palak (spinach) again." These foods do contain the substance that goes into the common stone, so families ban them completely. My advice is much simpler: eat normally, just do not overdo any one thing. If you are eating a huge amount of palak every day, ease off. But you do not need to give these foods up for life. (There is a small group of people whose stones start in childhood because of a problem they were born with, and they do need special testing. For everyone else, normal eating is fine.)
Myth: "Beer flushes the stone out." A young man will often ask me this, a bit shyly. Here is the truth:
"A bottle of beer and a bottle of water do exactly the same thing for a stone: they give you fluid. The only 'advantage' of beer is that people happily drink more of it. But alcohol actually dries you out. It makes you pass extra urine, so you feel like you are drinking plenty while your body is quietly getting more dehydrated."
If you do drink, drink plain water alongside it.
Myth: "Any cold drink counts as water." Be careful with canned drinks and juices. Sugary, packaged drinks are the wrong way to stay topped up with water. Fresh juice is fine. Canned and fizzy drinks are not. Plain water beats all of them.

Three common myths, and what is actually true: keep your dairy, water beats beer, and tomato and spinach are fine in moderation.
Myth: "The medicine dissolves or breaks the stone." It does not. No ordinary tablet melts or breaks a stone. The "stone-passing medicine" (usually tamsulosin) simply relaxes and widens the urine pipe (the ureter) so a small stone can slide out on its own. The stone leaves whole, in your urine; the medicine just smooths the road. Actually breaking a stone needs a laser or a procedure, not a pill.
What to actually eat and drink
The one word that matters most here is water. The best defence your body has is to keep flushing the system out. A small stone, caught while it is still small, often washes out on its own if the urine is watered down. The bigger a stone grows, the harder it is to pass, so pale, watery urine every day is the whole prevention plan.
A simple way to check you are drinking enough: your urine should stay pale, almost clear, through the day. If it turns dark yellow, you are behind. Drink more. Drink extra in summer, while fasting, and any time you are sweating or out in the sun. Carry a bottle. Do not wait until you feel thirsty. By then, you are already low.

A quick self-check: pale urine means you are well hydrated; dark means drink more.
Beyond water, the food advice is gentle and easy:
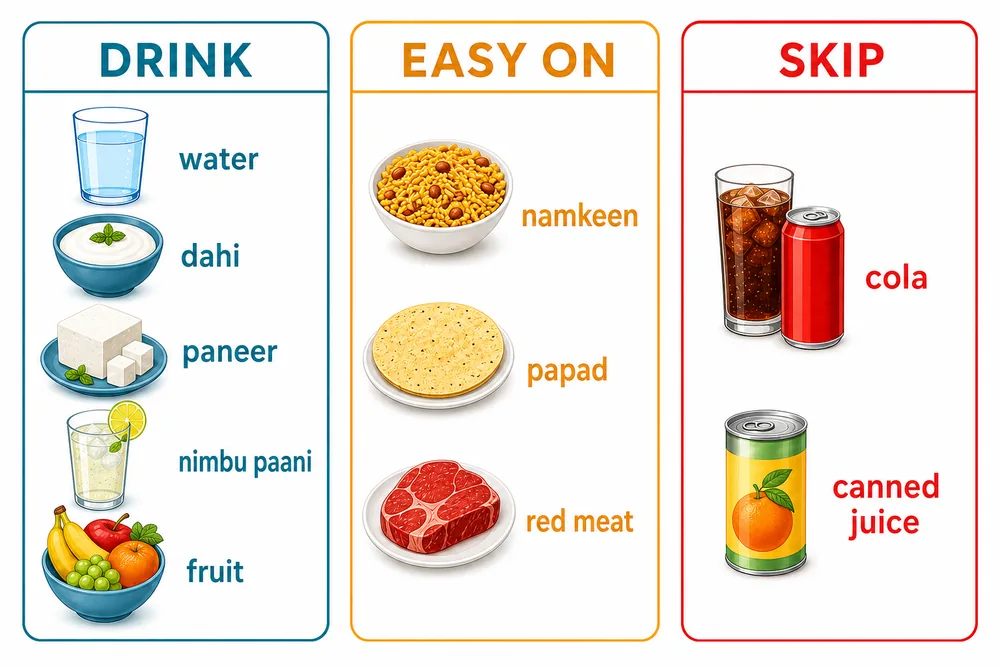
A simple plate guide: drink water and dahi, go easy on namkeen and red meat, and skip canned drinks and juices.
Why stones come back, and the patients I never see again
I wish I could promise no one ever gets a second stone. Some people are simply built to form them. It can run in the family, and sometimes the real cause is a problem in how the body handles its minerals, what doctors call a metabolic problem. This can be something you were born with: when the body mishandles oxalate from birth, stones often start in childhood, which is why any child with a stone gets full testing.
This is exactly why we send every stone for analysis. The chemical the stone is made of points to the specific fault in your body chemistry that created it. A calcium-based stone, for example, points us toward how you handle calcium, or to a small gland in your neck that controls your calcium levels, called the parathyroid. Once we know the fault, we can often correct it with medicine aimed at that exact problem, instead of just hoping the stone does not come back. For anyone whose stones keep returning, that testing is what finally breaks the cycle.
"The body's own best defence is to flush things out. A small stone, while it is still small, you can flush out. The bigger it gets, the harder that becomes. So catch it early, and keep flushing."
But for most people, the difference between coming back again and again and never needing me again comes down to that one habit. The patients I almost never see a second time are the ones who took the water message seriously and kept their urine watered down, day after day. It sounds too simple to matter. It is the single thing that works best.
When to see a urologist
See a urologist if you have one-sided back or stomach pain, blood in your urine, a stone that will not pass, stones that keep returning, or you simply want a plan to prevent the next one after your first. One thing worth knowing: a stone is not always gone just because the pain has stopped. Sometimes the pain settles while the stone stays and quietly damages the kidney, so it is worth getting checked either way.
Dr. Anirudh is a urologist who treats stones and performs the procedures himself, and he consults in two places. In Delhi, you can see him at Holy Family Hospital. In Gurgaon, you can see him at Dr. Deepika's Complete Family Clinic. Whichever you choose, the same surgeon looks after you from the first scan to the treatment to the plan that keeps stones from coming back. You can read more about our kidney stone treatment in Delhi and Gurgaon here.
If there is one line to carry away: keep your urine watered down every day, and never ignore a one-sided pain.
Written by Dr. Anirudh Kaushik
Urologist, Dr. Deepika's Complete Family Clinic, Gurgaon, and Holy Family Hospital, Delhi.
A note: This page is general information to help you understand kidney stones. It is not medical advice for your particular case. Please follow the advice your own doctor gives you. If your symptoms change or get worse, or you are worried, contact Dr. Deepika's Complete Family Clinic. Last reviewed by Dr. Anirudh Kaushik.
Sources
This article is based on the major international kidney-stone treatment guidelines and on published medical studies, including research from Indian hospitals. The main ones:
- American and European urology associations: official guidelines on treating and preventing kidney stones (2014 and later).
- A 2023 medical review summarising how kidney stones are diagnosed, treated and prevented (American Journal of Kidney Diseases).
- Borghi and colleagues: a 5-year study showing that drinking more water roughly halves the chance of a stone coming back (1996), and a study showing a normal-calcium, low-salt diet works better than cutting calcium (2002).
- Curhan and colleagues: a large study showing that normal calcium in food lowers stone risk, it does not raise it (1993).
- Taylor and colleagues: a healthy, vegetable-rich eating pattern is linked to fewer stones (2009).
- Ferraro and colleagues: sugary soft drinks raise stone risk, while water, tea and coffee lower it (2013).
- Smith-Bindman and colleagues: ultrasound is a good first scan for suspected stones (2014).
- Indian research on what stones are made of and how common they are, from hospitals in Delhi and northern India (2005 and 2023), and a study linking heat exposure to stones in Indian workers (2020).

